

Mastectomy for Breast Cancer
Breast cancer surgery generally falls into two main categories:
Mastectomy
Breast-conserving surgery (wide local excision or lumpectomy)
This page provides information for patients who are considering, or have been advised to undergo, a mastectomy as part of their breast cancer treatment.
What Is a Mastectomy?
A mastectomy involves the complete removal of the breast, including the nipple and most of the skin. It is the most extensive form of breast cancer surgery and accounts for approximately 20% of breast cancer operations.
The aim of a mastectomy is to remove all breast tissue, leaving only the skin overlying the chest wall muscles. Not all patients are suitable for breast-conserving surgery, and in these situations, mastectomy is the recommended option.
Most patients undergoing mastectomy do not require radiation therapy. However, radiation may still be recommended if high-risk features are present, including:
Tumours larger than 5 cm
Involvement of the skin or chest wall muscle
Multiple involved axillary lymph node
When Is a Mastectomy Needed?
A mastectomy may be recommended for several reasons, including the following.
Large Tumours
If a tumour is larger than 5 cm, or cannot be removed without significantly affecting breast appearance, chemotherapy may be used first to shrink the tumour. If this is not successful, mastectomy may be required.
Aggressive Cancer Types
Some breast cancers carry a higher risk of recurrence following lumpectomy, making mastectomy the more appropriate option.
Failed Breast-Conserving Surgery
If a lumpectomy does not achieve clear margins (adequate healthy tissue around the tumour), mastectomy may be recommended.
Multiple Tumours
When cancer is present in multiple areas of the breast, mastectomy ensures that all disease is removed.
Inability to Have Radiation Therapy
Breast-conserving surgery requires postoperative radiation therapy. If you have previously had radiation or cannot receive radiation, lumpectomy is not suitable due to a significantly increased risk of recurrence.
Risk Reduction
For patients with a BRCA gene mutation or a strong family history of breast cancer, mastectomy may be recommended to significantly reduce future cancer risk. This is often combined with breast reconstruction.
Mastectomy vs Lumpectomy – Which Is Better?
There is no single “best” operation for all patients. The choice between mastectomy and breast-conserving surgery depends on individual circumstances.
For small tumours, mastectomy usually provides little additional survival benefit compared with breast conservation. In certain situations, however, mastectomy is necessary.
In general:
The risk of recurrence after mastectomy is approximately 0.5–1% per year (2.5–5% over five years)
The risk after breast conservation is approximately 1–1.5% per year (5–7% over five years)
This small difference means many women can safely choose breast-conserving surgery.
The decision is ultimately yours. Some patients prefer mastectomy to avoid radiation therapy, but this is a personal choice that should be discussed carefully with Dr Green. A mastectomy cannot be undone, whereas breast conservation preserves mastectomy as a future option if required. Many women who rush into unnecessary mastectomy later report regret.
Types of Mastectomy
Are All Mastectomies the Same?
There are several types of mastectomy. Not all options are suitable for every patient, and Dr Green will discuss the advantages and disadvantages of each.
Total Mastectomy
Removal of the entire breast, including the nipple and most of the skin.
Subcutaneous Mastectomy
Removal of all breast tissue and the nipple while preserving most of the skin. This is usually performed in combination with breast reconstruction.
Nipple-Sparing Subcutaneous Mastectomy
Similar to subcutaneous mastectomy, but the nipple is preserved where it is safe to do so.
Chemotherapy After Mastectomy
Does a Mastectomy Allow Me to Avoid Chemotherapy?
No. The decision to recommend chemotherapy is based on tumour biology, not the type of surgery performed.
Chemotherapy is commonly recommended for:
Tumours larger than 2 cm
High-grade (Grade 3) cancers
Involved lymph nodes
Younger patients (under 40 years)
Aggressive subtypes such as HER2-positive or triple-negative breast cancer
Double Mastectomy
Do I Need to Remove Both Breasts?
For most patients, removing the unaffected breast does not provide additional cancer benefit. Modern reconstructive techniques allow excellent symmetry following a single mastectomy.
The risk of cancer in the opposite breast at diagnosis is only 1–2%. Both breasts are carefully assessed with imaging once breast cancer is diagnosed. Lobular breast cancer carries a slightly higher risk, and MRI may be used for more detailed assessment.
A double mastectomy may be considered for patients with:
A strong family history of breast cancer
High-risk genetic mutations (BRCA1, BRCA2, CDH1, ATM, CHEK2)
The decision is always yours. There is no urgency, and removal of the other breast can be considered later if needed.
Recovery After a Mastectomy
What’s Involved?
A mastectomy is performed under general anaesthetic. You will usually be admitted on the day of surgery, with no special pre-operative preparation required.
Once asleep, the operation takes approximately 60–90 minutes, longer if breast reconstruction is performed.
During surgery:
An incision is made around the breast
All breast tissue is removed
Lymph node surgery may be performed if required
The skin is closed flat, leaving a scar approximately 8–10 cm long
One or two drains are usually placed
Post-Mastectomy Recovery
What Happens After My Operation?
You will usually stay in hospital for two nights. You may go home with a drain in place. Nursing staff will show you how to care for the drain and record fluid output.
Drains are typically removed after 1–2 weeks. Without a drain, fluid may collect under the wound (seroma), which would require needle drainage.
You will return to see Dr Green approximately one week after surgery to:
Review pathology results
Discuss any additional treatment
Have dressings removed
Breast Reconstruction After Mastectomy
Is This an Option?
Breast reconstruction is an important topic to discuss prior to mastectomy. Reconstruction may be performed:
Immediately at the time of mastectomy
Delayed to a later date
Options include reconstruction using your own tissue (such as abdominal tissue) or implants. Each option has advantages and limitations.
Eligibility for reconstruction depends on factors such as:
Breast and body shape
Smoking status
Need for post-operative radiation therapy
Dr Green will guide you through all available options during your consultation.
Possible Complications of a Mastectomy
Mastectomy is a commonly performed operation, and most patients recover well and leave hospital feeling comfortable within 1–2 days. However, as with any surgery, complications can occur.
More Common (up to 10–15%)
Fluid collection under the skin (seroma)
Bruising
Excess skin at the sides of the scar (“dog ears”)
Numbness over the chest wall and nipple (if preserved)
Uncommon (up to 5%)
Poor wound healing or wound edge necrosis
Wound infection
Bleeding requiring a second operation
Blood transfusion
Rare but Important (up to 1%)
Anaesthetic complications
Allergic reactions
Large areas of skin necrosis
This list is a guide and not exhaustive. Please discuss any concerns with Dr Green during your consultation.

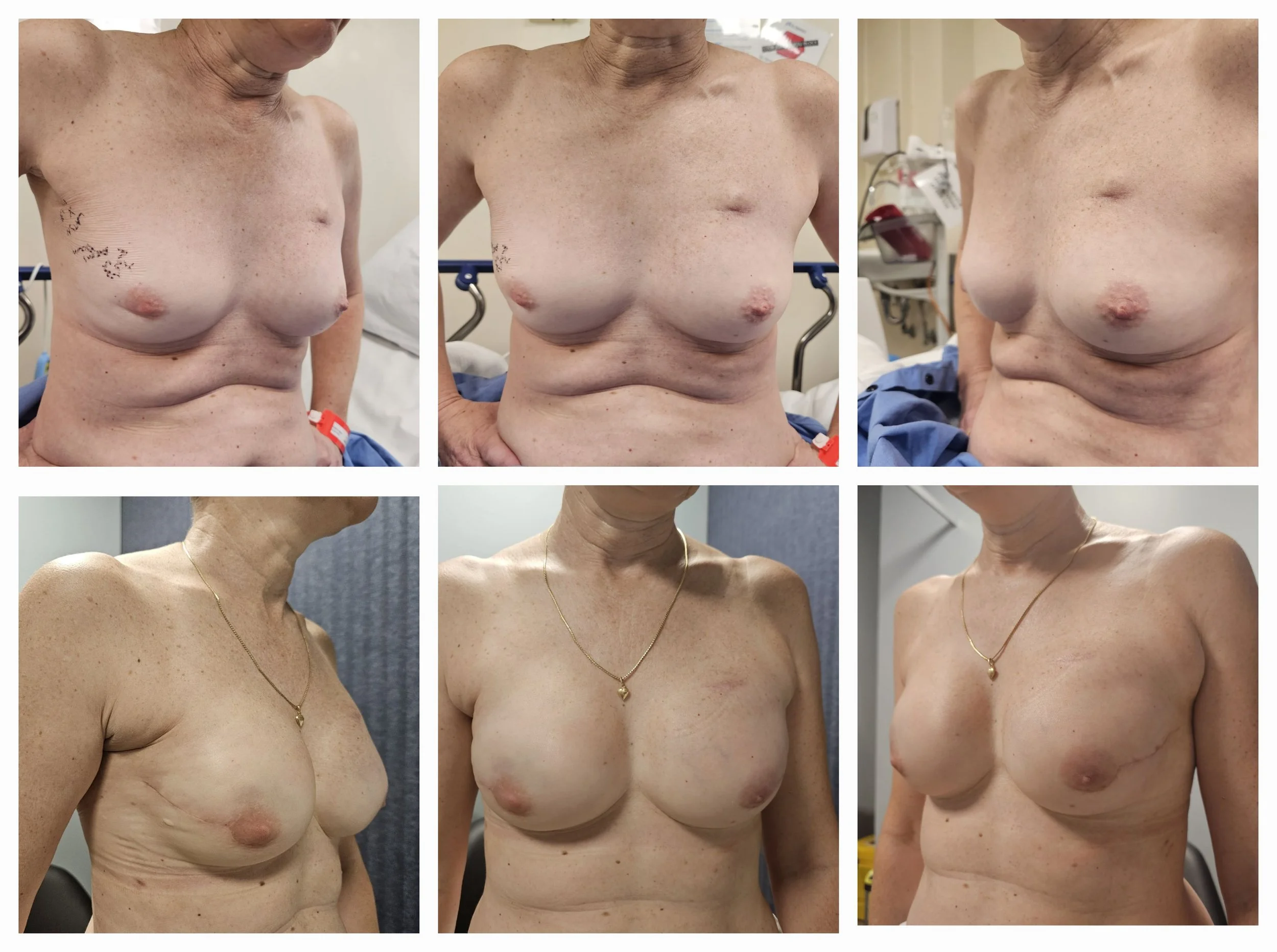
Immediate Implant Based Reconstruction following Nipple sparing mastectomy